What is bladder cancer and what are the causes?
Bladder is a spherical, hollow, muscular organ which stores and discharges the urine transported via ureters from kidneys. The inner part of this sphere is lined by a thin layer of cells called the epithelium (urothelium) and malignant tumors arising from there are entitled as bladder cancers. Bladder cancer is encountered in males more often than females and usually affects elderly. Etiam non quam lacus suspendisse faucibus interdum posuere lorem ipsum. Sed velit dignissim sodales ut eu sem integer. Pulvinar elementum integer enim neque volutpat. Pretium aenean pharetra magna ac placerat vestibulum lectus mauris ultrices.
Smoking and tobacco use is the predominant cause for developing bladder cancer.
Occupational exposure to the production of certain chemicals as dyes, rubber, textiles and pesticides, fossil and carbon containing fuels and arsenic, chronic irritation of the bladder epithelium, exposure to radiation and certain types of parasitic infections as schistosomiasis are the other known causes of bladder cancer.
Symptoms
The most frequent complaint is painless hematuria (blood in urine) which may or may not cause changes in urine color. Other symptoms as pain or burning on urination (dysuria) and clots in urine and irritative voiding symptoms might be encountered. Blood in urine may be apparent; however, in most cases urine color turns to pink or orange and sometimes no discoloration occurs and blood in urine could be detected in a urine test (urinalysis).
In advanced cases where a bladder cancer has remained undetected and spread other parts of the body symptoms might include difficulty to urinate, unilateral lower back pain, weight and appetite loss, fatigue, swelling in the legs and pain on bones.
Diagnosis
In most cases abdominal or specifically urinary system ultrasonography reveals a mass in bladder easily. This is a non-invasive radiological investigation which does not require preliminary measures. Occasionally an abdominal computerized tomography (CT) may be necessary for initial diagnosis.

In cases when these investigations do not suffice for diagnosis and suspicion of bladder cancer persists an endoscopic procedure -cystoscopy is performed by a urologist. A thin instrument equipped with camera and video system is inserted into the bladder through the urethral opening and the inner part of bladder is inspected under direct visualization.
Figure 2 shows the appearance of bladder cancer during cystoscopy.
What’s next after initial diagnosis?
Initial intervention after diagnosis is to perform a TransUrethralResection (TUR) - BT of bladder tumor. This is a procedure performed under general or spinal anesthesia (the lower part of the body is numbed) in the operating room. Patients are scheduled early in the morning to complete preliminaries for the procedure. Surgery is performed the same day by inserting special instruments attached to a camera into the bladder through urethra. All visible tumor tissues and specimens containing entire muscle layers of bladder near the tumor are resected and removed. These samples are sent to pathology lab to microscopic diagnosis. Subsequently a urethral catheter is inserted to drain urine and control bleeding and the patient is brought back to bed. Patients are mobilized on the day after and urethral catheter is usually removed on the second or third day before discharge.
Why TUR-BT Surgery so important?
TUR of bladder tumor confirms precise diagnosis of cancer and reveals pathological features defined as grade of the tumor (Low Grade-G1; High grade-G3) and the depth of tumor invasion through the layers of bladder wall as pTa, Pt1 or pT2, pT3. pTa defines a superficial tumor where the depth of invasion increases to the most inner muscle layers as it is referred to be pT3. With this approach we can define the cancer with all its features including its grade and stage which reveals the aggressiveness. Furthermore, this procedure may be sufficient for definitive treatment of some bladder cancer patients.
To obtain these valuable information, surgeon experience is of importance. When performing TUR for bladder tumor, surgeon must be able to remove all visible tumor (sometimes this may not be possible and a second procedure after a certain time is mandatory) and should take deep muscle samples of bladder without perforating it. Tumors over 3 cm in size requires great experience.
Terms that may be encountered in pathology reports to understand bladder cancer and treatment
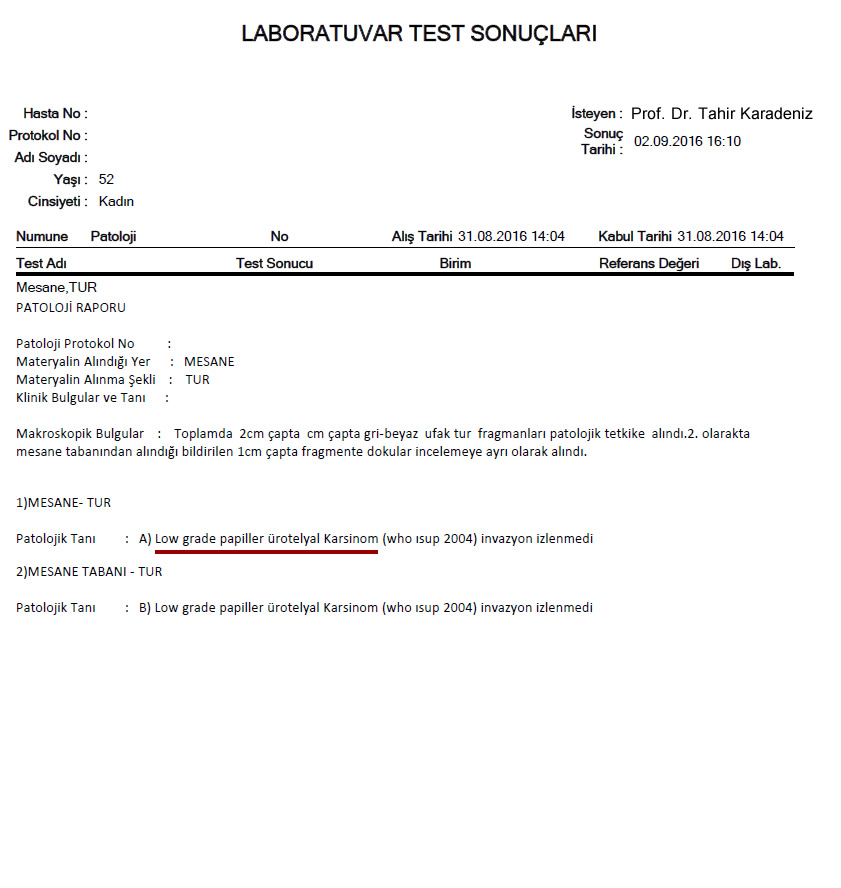
- pTa Low Grade – pTa Gl: This is the type of bladder cancer confined to the superficial layer of mucosa lining the most inner part and does not have aggressive potential to invade deep layers of bladder.
- pTa High Grade – pTa Glll: This type is very aggressive and has great potential to invade deep layers but not yet. Though this type carries high probability of spreading to distant organs of the body (metastases), fortunately it is rare.
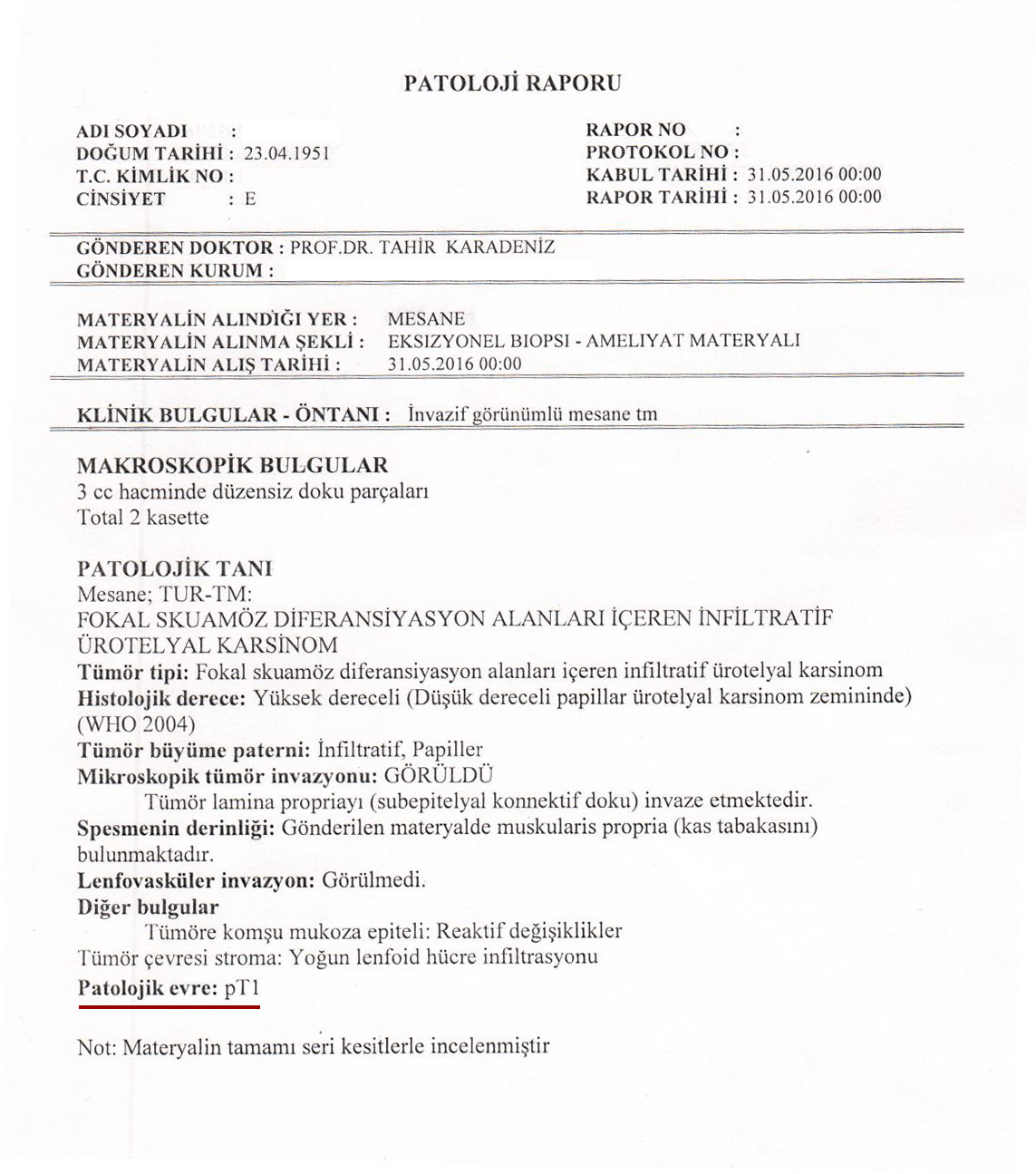
- pT1 High Grade – pT1 Glll: When compared to Ta, these cancers are very aggressive and have already invaded deeper layers of bladder without compromising bladder muscle. They have the potential to spread distant organs and lymph nodes.
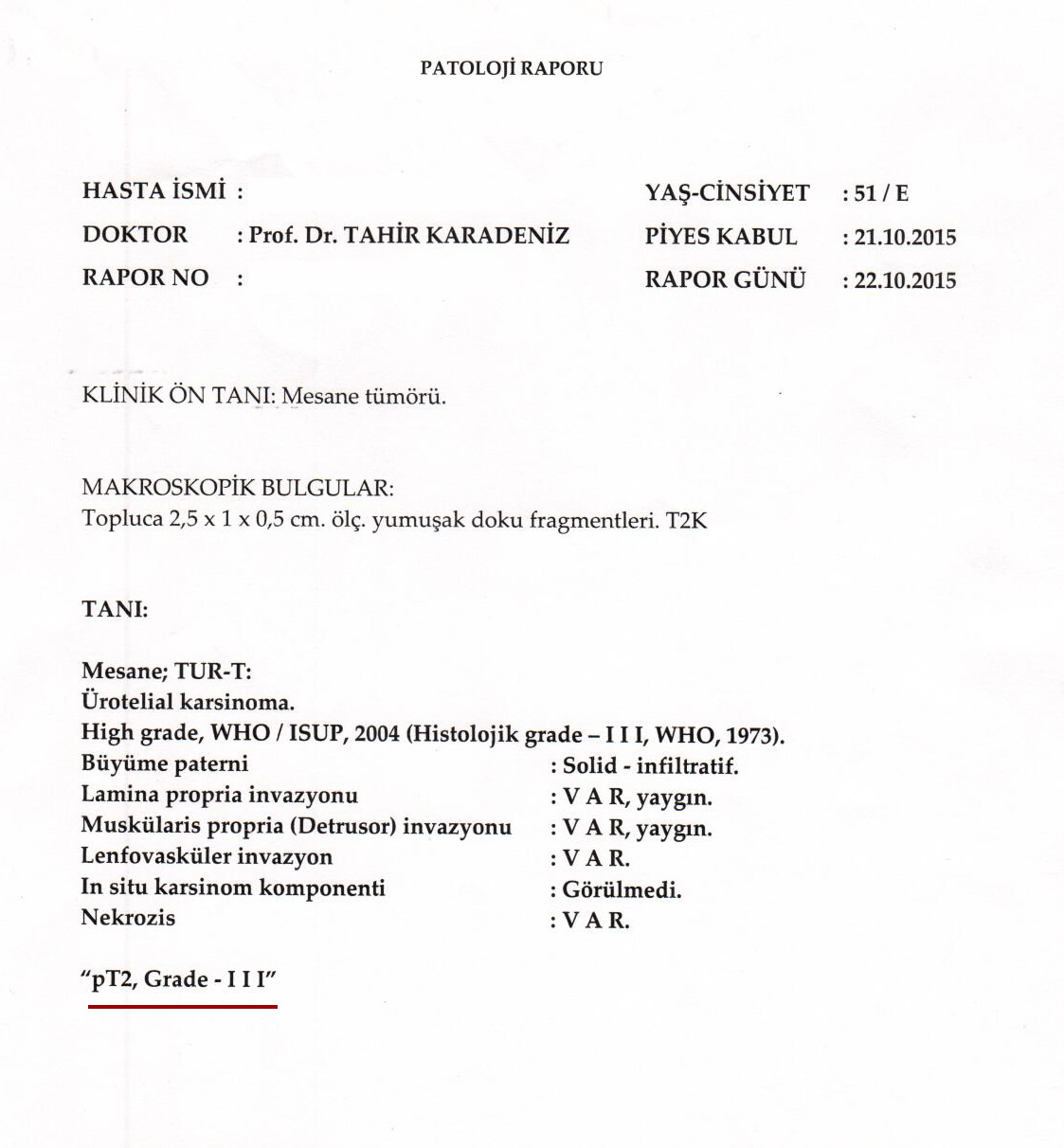
- pT2 High Grade – pT2 Glll Cancers which have already invaded bladder muscle and may extend outside with high aggressiveness; when delayed, spreading potential to lymph nodes, lungs, liver and bones is likely.
In the section below, you can find examples of pathology reports and interpret better.
Treatment of Bladder Cancer
Treatment of bladder cancer depends entirely upon the pathological report of initial TUR-BT operation. Once the report is obtained, management options are regarded according to the pathology result. We find it more proper to describe by examples, so that patients who have undergone initial TUR-BT for bladder cancer can find his case in the following instances.
- Example 1) pTa Low Grade – pTa Gl: When pathology yields a bladder cancer as pTa Gl and the size of the cancer is below 3 cm, a perfect surgery performed by an experienced surgeon is sufficient for treatment in most cases. Intravesical weekly instillations of certain drugs may be considered after a joint decision with the patient. Follow up cystoscopies are carried out at certain intervals (every 3 months in the first year) against the possibility of recurrence. A TUR-BT is carried out again whenever recurrence is discovered.
- Example 2) pTa Low Grade – pTa Gl: If the tumor size is over 3 cm or more than 1 tumor is resected, a repeat TUR-BT is performed 2-4 weeks after initial surgery to achieve complete resection. Subsequently, certain drugs are administered intravesically for 6 weeks and follow-up cystoscopies are scheduled.
- Example 3) pTa High Grade – pTa Glll: If pathology reports such a consequence, a repeat TUR-BT operation is performed 2-4 weeks(re TUR ) after whatever the size of initial tumor happens to be. Ultimate management is based upon the second pathologic evaluation. This type of bladder cancer is very aggressive and has high potential to disseminate. Intravesical administration of BCG (Bacillus Calmette Guerin; vaccine against tuberculosis) is carried out according to a schedule if tumor size is smaller
Then 3 cm and only one tumor
If the tumor size is karger then 3 cm, and/or multipl tumors, if the tumor/s unresponsive to intravesical BCG treatment
Radical CYSTECTOMY can be offered and it CAN BE LİFE SAVİNG SURGERY
- Example 3) pTa High Grade – pTa Glll: If pathology reports such a consequence, a repeat TUR-BT operation is performed 2-4 weeks(re TUR ) after whatever the size of initial tumor happens to be. Ultimate management is based upon the second pathologic evaluation. This type of bladder cancer is very aggressive and has high potential to disseminate. Intravesical administration of BCG (Bacillus Calmette Guerin; vaccine against tuberculosis) is carried out according to a schedule if tumor size is smaller
- Example 4) pT1 High Grade – pT1 Glll: A repeat TUR-BT must be performed 2-4 weeks after initial operation when pathology indicates a pT1Glll tumor; namely, initial surgery should be repeated (re TUR ) This surgery is named as re-TUR-BT in urologic terminology. The purpose is to discover an unrevealed pT2 cancer which has invaded deep into the bladder muscle and could not been exposed in the first TUR-BT. If it is found out to be as pT1 Glll in accordance with initial report and a low volume of tumor is present, weekly intravesical BCG instillations are scheduled. When tumor burden is too high, Radical Cystectomy – removal of bladder, prostate and seminal vesicles (in the male) – ovaries, uterus and part of vagina (in the female) are removed along with regional lymph nodes – may be performed.
Then 3 cm and only one tumor
If the tumor size is karger then 3 cm, and/or multipl tumors , if the tumor/s unresponsive to intravesical BCG treatment
Radical CYSTECTOMY can be offered and it CAN BE LİFE SAVİNG SURGERY
- Example 4) pT1 High Grade – pT1 Glll: A repeat TUR-BT must be performed 2-4 weeks after initial operation when pathology indicates a pT1Glll tumor; namely, initial surgery should be repeated (re TUR ) This surgery is named as re-TUR-BT in urologic terminology. The purpose is to discover an unrevealed pT2 cancer which has invaded deep into the bladder muscle and could not been exposed in the first TUR-BT. If it is found out to be as pT1 Glll in accordance with initial report and a low volume of tumor is present, weekly intravesical BCG instillations are scheduled. When tumor burden is too high, Radical Cystectomy – removal of bladder, prostate and seminal vesicles (in the male) – ovaries, uterus and part of vagina (in the female) are removed along with regional lymph nodes – may be performed.
- Example 5) pT2 High grade- pT2 Glll: Radical Cystectomy is the choice of treatment when initial pathology reveals a pT2 Glll bladder cancer if the condition of the patient is suitable for such a surgery.
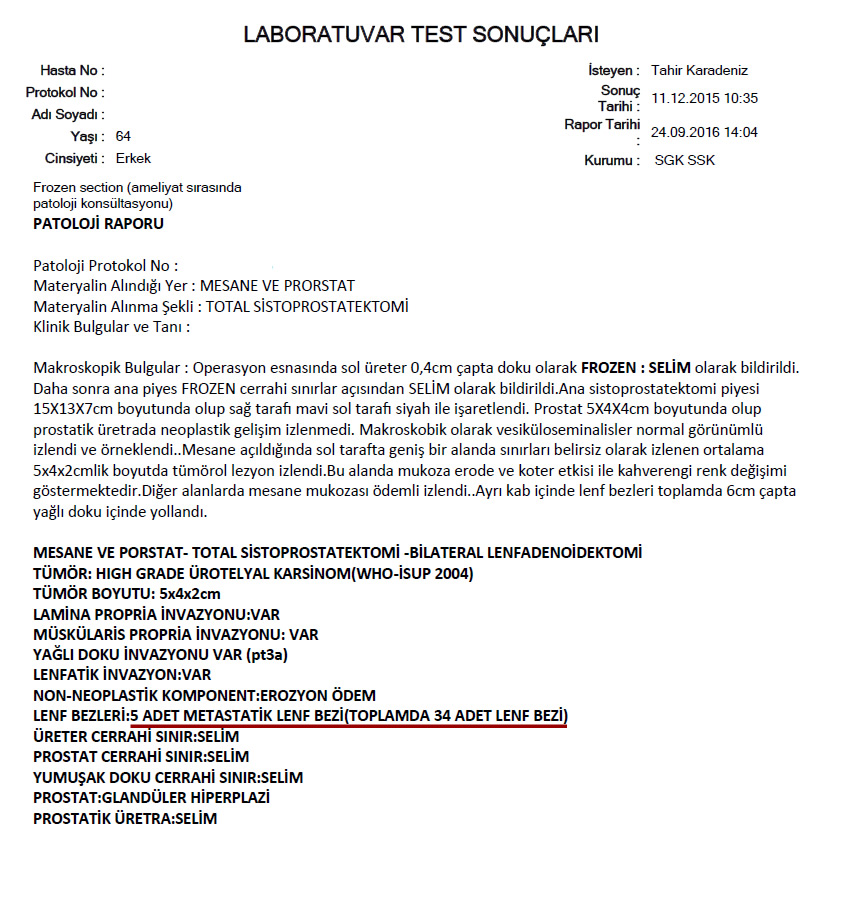
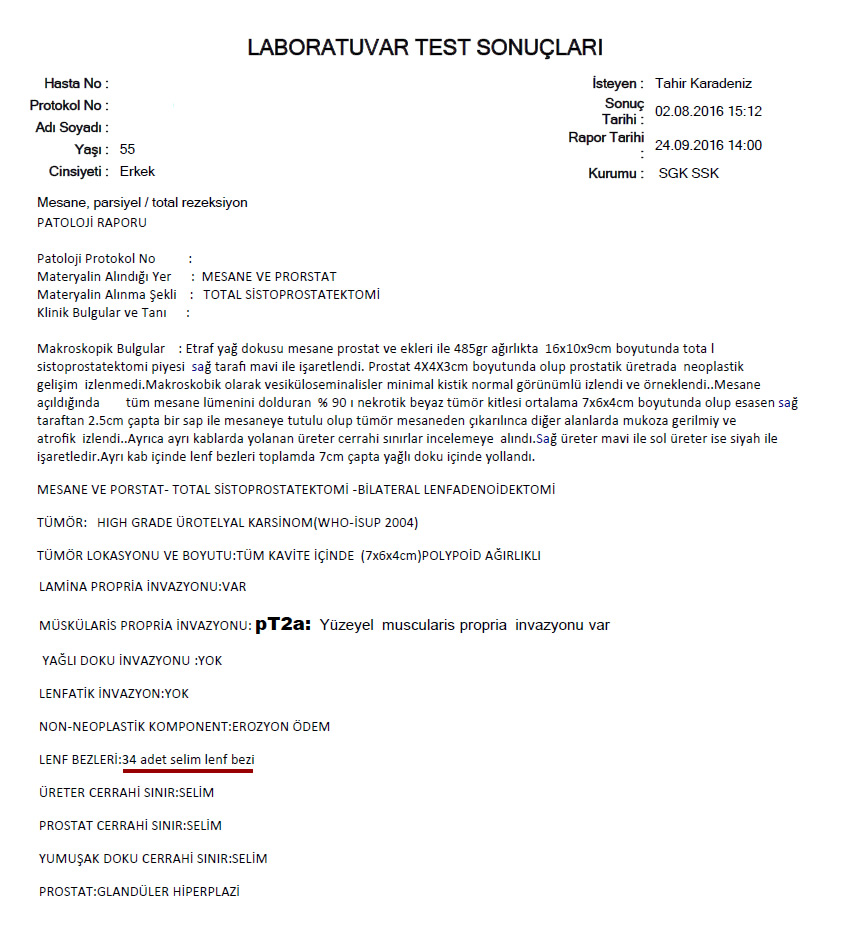
Examples of Pathology Reports After Surgery for Bladder Cancer
What Is Radical Cystectomy Surgery?
This is a major surgery in urology and should be performed after proper handling of preoperative requisites. During this operation bladder is removed entirely together with a part of lower urinary tract (ureters), prostate and seminal vesicles (in men) and uterus, ovaries and part of vagina (in women) along with the lymphatic tissue surrounding great vessels. Duration of a complete performance of radical cystectomy is between 6 and 8 hours. When necessary, the patient is followed in the intensive care unit for 24 hours after the surgery and taken to his room the day after. As oral intake would not be possible for 2 or 3 days parenteral nutrition with special solutions is initiated. Usually the patient is discharged between 10 to 14 postoperative days.
What Is the Importance of Removing Lymph Nodes and The Significance of The Number of Lymph Nodes?
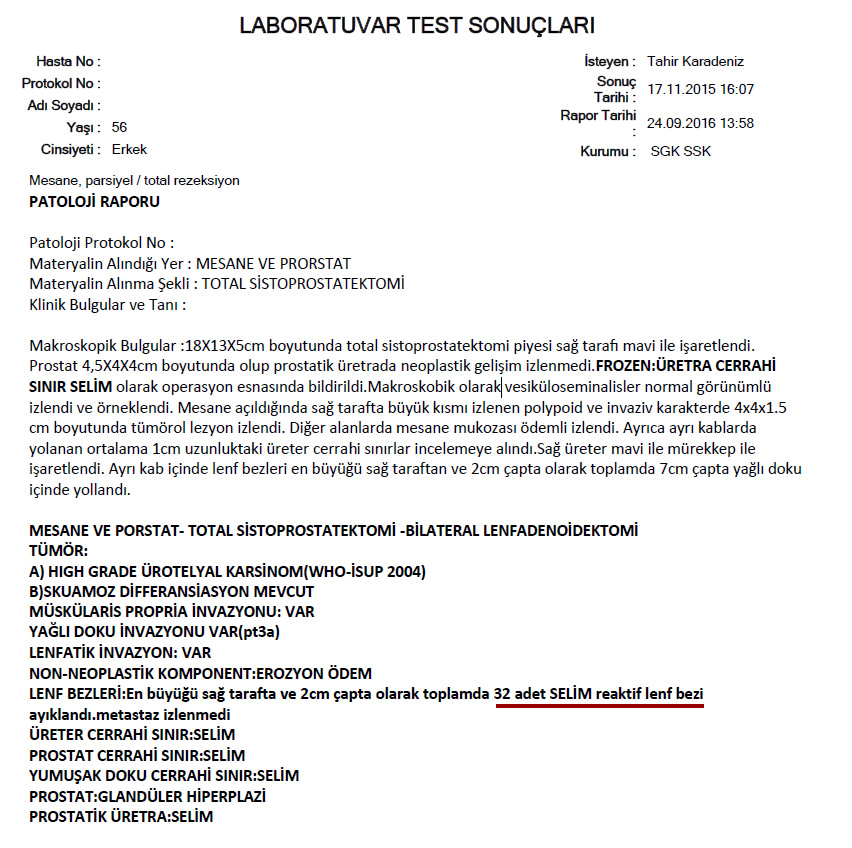
This is the crucial part of radical cystectomy surgery. Because resection of lymph nodes requires special training and experience most urologic surgeons omit lymph node dissection. However, presence of cancer in lymph nodes could be detected thus the extent of cancer and the need for further chemotherapy be understood precisely. Additionally, it is an established data that the more the number of resected lymph nodes means increased expectancy in the rate of patient survival.
Below you can find the number of resected lymph nodes in pathology reports of our patients.
You can read our published data in a respected journal reporting the effect of the number of resected lymph nodes to the life span among bladder cancer patients:
Link: http://www.ncbi.nlm.nih.gov/pubmed/21910098
We documented that when increased number of lymph nodes is removed a longer and better quality of life can be offered to bladder cancer patients.
What Is “Neobladder” Surgery?
This means the construction of a “new bladder” from a portion of small bowels after removal of all the bladder. The intention of this surgery is to provide a better quality of life by maintaining micturition in the natural way through native urethral meatus. After a portion of small bowel is harvested and shaped into a sphere, ureters from both kidneys is anastomosed to the proximal part of this segment. The most prominent part of this sphere is attached to native urethra thus providing urination normally. This is a complex surgery requiring special training and skill. Our team has gained great experience perhaps the most in Istanbul with hundreds of “neo-bladder” surgery cases.
We remove the urethral catheter between 12. postoperative day and educate the patient how to empty the new-bladder. If the patient wishes, we request our former patients with a new-bladder to meet so that they can share their experience during rehabilitation period. It usually takes 4 to 5 days for the patient to learn how to urinate with the new-bladder.
What is Orthotopic Neobladder? animation video
Urination After Radical Cystectomy?
After a radical cystectomy surgery, a new way must be created for urine to leave the body (urinary diversion). There are three options for urinary diversion:
Ileal Conduit: Using an average of 15 cm part of small intestine a small tube which drains urine outside the body is created. Ureters are attached to the proximal end and the distal portion of the tube is brought out abdomen where the patient wears a urostomy bag collecting urine. The bag is emptied either by the patient or the caregiver when it is full of urine.
Continent Urinary Reservoir: This is a reservoir formed with a segment of small bowel inside the body to collect urine. The patient drains this reservoir several times a day by a catheter through the opening in the abdominal wall.
Neobladder Construction: After radical cystectomy the ideal solution for taking urine out of the body is to create e new bladder that will store and evacuate urine. This can be accomplished by creating a neobladder using the patient’s small bowel. A segment of intestine is excised and formed into a sphere to collect urine. The ureters transporting urine from kidneys are attached to one end of this intestinal segment and the distal part is anastomosed to the patient’s own urethra. This eliminates either the need to wear any bag to collect out of the body or catheterization for several times a day. This surgery is named after Orthotopic Bladder in urology.
Follow-up After Surgery
As with other cancers follow-ups are scheduled at 3 months intervals in the first 2 years and at 6 months intervals then after for 5 years.
The Role of Chemotherapy in Bladder Cancer Treatment / To Whom / When?
We can define the extent of cancer in patients referred with high grade bladder cancer by performing radiologic studies including CT Urography and CT of Thorax and diagnose extravesical disease (adjacent lymph nodes, rectum, distant organs as lungs, liver and bones). In such circumstances chemotherapy is preferred as initial therapy. When performed prior to surgery, it is referred as Neoadjuvant Chemotherapy. After neoadjuvant chemotherapy when distant spread of the disease (metastases) disappears or a decrease in extravesical spread is noted surgery may be performed.
Surgery is primarily performed when no extravesical extension or spread to distant organs exist. Chemotherapy is scheduled if lymphatic involvement or invasion of perivesical fat tissue with cancer cells is found on pathologic examination after surgery. Chemotherapy following surgery is named as Adjuvant Chemotherapy.
If cancer cells are found to invade outer layers of bladder or metastases to the removed lymph nodes are present patients are referred to chemotherapy. If these two main features are absent there exists no need for chemotherapy. During follow up chemotherapy programs may be initiated if distant organ (lungs, liver, bones or intraabdominal spread) involvement or local recurrence is found.